All published articles of this journal are available on ScienceDirect.

Hypnotherapy, Relaxation, and Music Therapy in Pediatric Cancer Pain Management: A Clinical Trial Comparison
Authors Info & Affiliations
Abstract
Introduction
Pain is a prevalent issue across various medical conditions, and numerous methods have been employed to manage it. In developed countries, cancer ranks as the second leading cause of mortality after cardiovascular diseases. This study aims to compare the effectiveness of hypnotherapy, relaxation therapy, and Music Therapy (MT) with control groups in alleviating pain in children with cancer.
Methods
The research involved a single-blind clinical trial with a study population comprising children diagnosed with an abdominal mass and acute lymphoblastic leukemia. Fifty-eight patients were selected through blocked randomization. Data were collected through a demographic checklist and the Visual Analog Scale (VAS) to measure pain intensity. Data analysis was carried out using repeated measures ANOVA in SPSS version 22 to compare mean pain intensity among the study groups.
Results
A total of 58 patients, with an average age of 9.28±4.02 years, participated in the study. Significant differences were observed between the hypnotherapy group and the other study groups (F=14.51; P≤0.001), as well as between the MT group and the other study groups (F=12.81; P≤0.001). Moreover, significant differences were found in terms of time between the relaxation therapy group and the other study groups (F=8.46; P≤0.001) and between the control group and the other groups (F=5.506; P≤0.001).
Conclusion
Based on the findings, relaxation therapy, hypnotherapy, and Music Therapy (MT) have shown significant effectiveness in alleviating pain in cancer patients during their treatment.
Clinical Trial Registration No
Trial registration Clinical trial. gov Identifier: IRCTID website (code: IRCT20120905010744N2; http://irct.ir).
1. INTRODUCTION
Cancer is characterized by its rapid growth rate and the spread of cancerous cells, known as metastasis [1]. In developed countries, it is the second leading cause of death after cardiovascular diseases [2]. According to the American Cancer Society (2013), over 1,660,000 new cases of cancer were diagnosed in 2015 [3]. The diagnosis and treatment of cancer can often be confusing for patients and their families, leading to significant stress that affects both psychological and physiological adaptations, including neuroendocrine changes [4]. These adaptations may influence tumor growth, the body's defense mechanisms, disease progression, and the overall quality of life of cancer patients [5].
Pain is a prevalent discomfort experienced by cancer patients, often originating from neuropathic sources due to tumor invasion affecting various parts of the nervous system [6]. Existing literature suggests that cancer pain can be effectively managed through multimodal therapies [7]. Among children with cancer, pain affects as much as half to three-fourths of the population [8]. Experts emphasize that an effective approach to managing pain in cancer patients involves a multifaceted strategy that integrates psychological, physical, interventional, and complementary therapies throughout the disease's course [9]. A separate study has demonstrated the pain-reducing benefits of hypnotherapy in cancer patients [10].
Hypnotherapy is a commonly used method for managing cancer-related pain, where hypnosis involves a collaborative effort between a hypnotist and a designated patient or client to achieve changes in feelings, perceptions, cognition, emotions, mood, or behavior [11]. Children diagnosed with cancer often undergo painful treatments that induce significant psychosocial distress [12]. Hypnotherapy has been shown to be beneficial in alleviating distress and pain in pediatric patients [13].
The integration of hypnosis into specialized oncology centers could offer significant benefits to cancer patients, especially children, in reducing pain [14]. In clinical practice, the optimal management of patient symptoms necessitates a holistic approach that combines psychological and medical interventions, making hypnosis a valuable addition to comprehensive care programs [15].
Music Therapy (MT) is another unconventional approach to managing cancer-related pain. Extensive research has indicated the profound impact of music on health, a concept rooted in traditional medicine worldwide [16]. Music specifically influences brain regions associated with motivation, cognition, emotions, and motor function [17]. Researchers have used music-based interventions to enhance emotional, cognitive, and neuromotor functions [18]. To effectively utilize its potential in cancer treatment, music's sociocultural, multifaceted nature must be delineated into specific, measurable parameters [19].
The brain's reward system plays a key role in regulating emotional states, pain reduction, and anxiety relief, and there is evidence supporting the effects of music on this reward system [20]. A meta-analysis reveals that music interventions significantly improve fatigue and pain in cancer patients, with a positive impact lasting for a minimum of 30 minutes [21]. Numerous studies have provided evidence of music's ability to reduce pain in cancer patients [22].
Relaxation is another approach suggested for managing cancer-related pain and reducing distress [23]. While relaxation exercises may require some time, they have been shown to produce optimal results within a relatively short period [24]. Many studies have affirmed the positive impact of relaxation exercises, particularly after 3-12 weeks [25].
Cancer patients often experience significant discomfort within 7-10 days of commencing chemo- therapy, and relaxation exercises, such as controlled breathing, contribute to muscle relaxation in the neck, shoulders, and upper chest [26]. This, in turn, enhances the breathing process and reduces physiological strain and stimulation. Previous studies have demonstrated that relaxation exercises lead to reduced neuromuscular activity, decreased sympathetic nervous system activity, and a lower excitability state in the cerebral cortex [27].
In light of these considerations, this study aims to compare the effectiveness of hypnotherapy, relaxation, and Music Therapy (MT) with control groups in relieving pain in children with cancer [28].
2. METHODS
This single-blind clinical trial obtained permission from the Vice Chancellor for Research of Kurdistan University of Medical Sciences to access cancer patients through the Head of the Cancer Department. The study adhered to the CONSORT guidelines [25]. The Consort flow diagram is presented in Supplementary material. The Visual Analog Scale (VAS) was used for all patients before the study. Additionally, the VAS was used in every session of the three intervention groups. The VAS was also used to control pain in children in a previous study [29].
2.1. Inclusion and Exclusion Criteria
2.2. Intervention Groups
2.2.1. Relaxation Therapy
Progressive Muscle Relaxation (PMR), introduced by Jacobson in the early 1900s, was employed to induce a physical relaxation response. PMR consists of four sessions, each completed within four days and lasting 30 minutes. This technique involves the sequential contraction and release of major muscle groups throughout the body [26].
2.3. Hypnotherapy
• Patients in the hypnotherapy group underwent four hypnosis sessions utilizing various approaches, including the dissociative technique, inductive technique, pain relief, distraction, and telescope technique [28]. The Erickson induction technique, Ideosensory technique, and deepening techniques were employed for pain relief and hypnosis induction [28].
It should be noted that hypnosis should be conducted by a specialist, as it may otherwise lead to detrimental results.
2.4. Music Therapy (MT)
• Participants were introduced to music and received MT based on their preferences. Different types of music, including Persian, classical, and traditional Persian, were selected. Music was delivered via Sony headphones for 3 to 30 minutes daily over four weeks. Pain intensity was assessed before and after the intervention using the Visual Analog Scale (VAS) [27]. Pre-recorded music was used [30].
2.3. Data Collection Tools
Pain intensity was assessed using a VAS with a ruler displayed on paper. Patients marked the scale to indicate their level of pain, ranging from zero (no pain) to ten (intolerable pain) [31].
2.6. Demographic Checklist
A demographic checklist was used to collect patient information, including age, education level, parental occupation status, and education level, as well as the group assigned to the study. Block randomization was used to assign patients to intervention and control groups.
The study included children aged 6-16 years diagnosed with acute lymphoblastic leukemia. The sample size of 58 pediatric patients was determined with a 5% alpha and 80% test power. The mean age of the patients was 9.28±4.02 years, calculated using the following sample size formula:
In total, 58 pediatric patients aged 6-16 years with acute lymphoblastic leukemia were enrolled in the study. Notably, the diagnosis had been confirmed by an oncologist at the oncology ward of Besat Hospital. The study started when the oncologist diagnosed the patients with cancer, i.e., none of the participants had received the analgesic before. The patients were allocated to the intervention and control groups via block randomization by a Professor of Vital Statistics. Initially, the block size was set at four based on the sample size, and the patients were assigned to each group by 14 blocks using the random number 1 considering the block positioning. The blocks required for this stage of the study were provided by the hospital's oncology ward.
The patients were allocated to three intervention groups. In the hypnotherapy intervention group, the protocol described in the method section was implemented by a doctoral graduate in pediatric and clinical psychology. Relaxation therapy was the second inter- vention group (method described earlier in the text), and the patients in the third intervention group received MT (method described earlier in the text). The patients in the control group received no intervention.
Also, to eliminate the internal control error, the outcome (pain) was recorded by the nurse in the oncology ward. She had no information about the outcome, and she was completely blinded, so the internal error was removed.
2.7. Ethical Considerations
The participants were assured of confidentiality terms regarding their information, and participation was free of charge. The research objectives were explained to the subjects verbally and in a written manner, and written informed consent was obtained before enrollment. Notably, the participants were allowed to withdraw from the study at any given time. The study protocol was approved by the Ethics Committee of the Kurdistan University of Medical Sciences (code: IR.MUK.REC. 1396.15), and the study has been registered on the IRCTID. Website: http://irct.ir (Code: IRCT201209050 10744N2).
3. RESULTS
Finally, 58 patients were included in the study, of which 34 were boys (58.6%) and 24 were girls (41.4%). The mean and standard deviation of the age of the patients in the three groups of hypnotherapy, relaxation, and music therapy were 9.37 ± 2.89, 9.23 ± 2.86, and 9.37 ± 2.89, respectively. This value was 8.12 ± 2.82 in the control group and was not statistically significant. Other demographic information of patients is demonstrated in Table 1. The relationship between the demographic variable and intervention group is demonstrated in Table 1.
As shown in Table 1, no significant differences were observed between the hypnotherapy, relaxation, MT, and control groups in terms of age (P≥0.05), gender (P≥0.05), father's job (P≥0.05), mother's job (P≥0.29), and respondents' education (P≥0.28).
Table 2 presents the results of the repeated-measures ANOVA analysis, comparing the mean reduction in pain among the studied groups at baseline, after one session, and after four sessions.
| - | - | Hypnotherapy | Relaxation | MT | Control | p |
|---|---|---|---|---|---|---|
| Gender | Male | 8(23.5) | 10(29.4) | 8(23.5) | 8(23.5) | P≥0.5 |
| Female | 8(33.3) | 3(12.5) | 5(20.8) | 8(33.3) | ||
| Father’s job | Staff | 5(50) | 2(20) | 2(20) | 1(10) | P≥0.5 |
| Self-employment | 11(26.2) | 11(26.2) | 7(16.7 | 13(31) | ||
| Unemployment | 0(0) | 0(0) | 4(66.7) | 2(33.3) | ||
| Mother’s job | Staff | 2(100) | 0(0) | 0(0) | 0(0) | P≥0.29 |
| Self-employment | 1(50) | 0(0) | 0(0) | 1(50) | ||
| Unemployment | 13(24.1) | 13(24.1) | 13(24.1) | 16(27.6) | ||
| Respondents ‘education | School Preparation Course | 12(28.6) | 10(23.8) | 10(23.8) | 10(23.8) | P≥0.28 |
| Elementary | 4(25) | 3(18.8) | 3(18.8) | 6(37.6) |
| Groups | Before | Before | After Week 2 | After Week 3 | After Week 4 | f | p |
|---|---|---|---|---|---|---|---|
| Hypnotherapy | 3.25±2.89 | 3.25±2.89 | 0.38±.46. | .63±1.48 | .41±1.23 | 14.5 | 0.001 |
| Music therapy | 3.38±1.97 | 3.38±1.97 | 1.65±1.09 | 1.69±1.98 | 1.08±1.05 | 12.8 | 0.001 |
| Relaxation | 3.65±2.10 | 3.65±2.10 | 2.28±1.94 | 1.80±1.72 | 1.38±1.85 | 8.46 | 0.001 |
| Control | 4.43±3.03 | 4.43±3.03 | 4.93±2.23 | 6.3±2.24 | 5.29±2.62 | 5.51 | 0.001 |
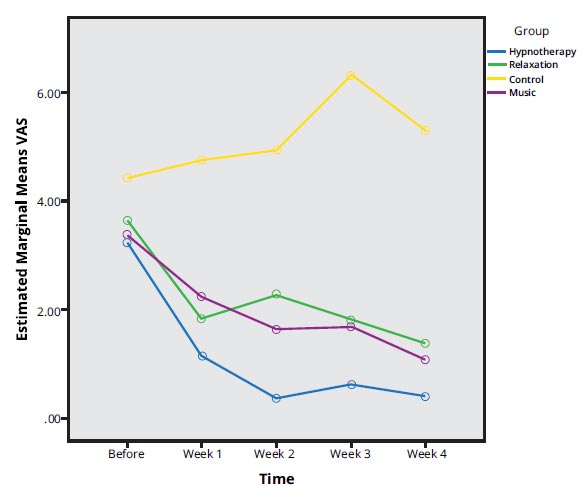
Mean pain severity in intervention and control groups (p<001).
In Table 2, significant differences were observed between the hypnotherapy group and the other study groups (F=14.51; P≤0.001). Similar findings were noted between the MT group and the other study groups (F=12.81; P≤0.001). Furthermore, Table 2 demonstrates a significant difference in pain reduction between the relaxation group and the other groups over time (F=8.46; P≤0.001). A similar finding was observed between the control group and the other groups in this regard (F=5.506; P≤0.001). Fig. (1). depicts the mean pain intensity in the control and intervention groups (P<001).
Fig. (1) shows that the three intervention groups:hypnotherapy, music therapy, and relaxatio, significantly reduced pain among cancer patients compared to the control group (p < 0.001)
4. DISCUSSION
The management of pain is one of the concerns in children with cancer. According to the findings of this study, pain intensity significantly decreased in pediatric cancer patients who received hypnotherapy, Music Therapy (MT), and relaxation when compared to the control group. Notably, the MT group experienced the most rapid pain relief after the intervention, which is consistent with the findings of Gramaglia et al. in 2019 [14], indicating the profound impact of music on brain regions responsible for motivation, emotions, motor functions, and cognition. In this study, the choice of music was culturally relevant to the Kurdistan province of Iran [32].
These results align with previous studies demonstrating the effectiveness of music in inducing intense pleasure in the brain's reward system and its direct impact on survival-related brain mechanisms [17]. Similar to our findings, previous research [14] has suggested that music can serve as a potent, cost-efficient, and easily applicable treatment method in various clinical settings and disease stages, supporting the potential of music therapy in clinical practice [6, 14-17].
Hypnosis has been widely employed to ameliorate complications caused by cancer, and our study's results support this approach [33]. We observed no significant associations between hypnosis and age, gender, ethnicity, or education level. This is in line with evidence demonstrating the acceptability of hypnosis among a majority of cancer patients [33]. While limited studies have focused on self-hypnosis and its effects on pediatric patients, it has been reported as effective when properly trained [34].
These results are consistent with findings from Miró and Tomé-Pires' study, which concluded that hypnosis is an effective method for pain control in children with cancer pain or chronic pain [11]. Similarly, the study by Wood and Bioy demonstrated the effectiveness of pediatric hypnosis for alleviating pain during medical procedures such as bone marrow aspiration and lumbar puncture, as well as reducing post-surgical pain and anxiety in children. Additionally, hypnosis has shown promise in managing headaches and other conditions, including chronic pain [35]. In a controlled, randomized trial conducted by Butler et al., it was concluded that hypnosis can reduce the intensity and duration of invasive medical procedures, such as Voiding cystourethrography, in children [36]. In contemporary cancer treatment, radiation therapy and chemotherapy play pivotal roles [1]. Hypnotherapy has gained attention as an integrated therapeutic approach to cancer treatment. In our study, the hypnotherapy group exhibited a more significant reduction in pain intensity compared to the control group, consistent with previous studies [1, 26, 37, 38]. The mechanism behind hypnosis's impact on pain likely involves neurophysiological processes within the pain matrix rather than a singular mechanism [39].
The third intervention group received relaxation therapy involving breathing exercises. Our results indicate that relaxation was effective in reducing pain intensity in pediatric cancer patients, aligning with the findings of Bordereau et al. in 2003, who also confirmed pain relief in cancer patients [40]. Additionally, relaxation and guided imagery have shown effectiveness in the management of cancer-related pain, as supported by similar studies [23, 24, 41, 42], which is in line with our results.
The present study's findings are consistent with those of Ting et al., who concluded that music therapy reduces postoperative and chronic pain in children [43]. Tulin-Silver et al. demonstrated successful pain management using music therapy during sclerotherapy in children with vascular malformations [44]. Additionally, Vagnoli et al. found that relaxation techniques are effective in reducing pain and anxiety before children's surgery [45]. Conversely, Olbrecht et al. showed that relaxin is effective in controlling pain and anxiety in children and adolescents with acute postoperative pain [46].
CONCLUSION
In conclusion, the results of this study suggest that Music Therapy (MT), relaxation, and hypnotherapy can effectively reduce perceived pain intensity in children undergoing cancer treatment. Hypnotherapy, in particular, appeared to have a more profound impact on participants, possibly due to its ability to enhance focus, accuracy, and control or reduce external stimuli. These approaches show promise for pain management in pediatric cancer patients. Healthcare professionals, especially nurses and clinical psychologists, may consider these alternative methods to address pain complaints in this patient population.
LIMITATIONS
One limitation of this study is the use of randomized block sampling, which may have led to variations in mental capabilities and disease tolerance among patients, potentially influencing their responses to music therapy, relaxation, and hypnotherapy interventions.
Another limitation is that we did not estimate the effects of these three interventions (music therapy, hypnotherapy, and relaxation) in conjunction with conventional analgesics. It is suggested that future studies investigate the effects of these interventions as adjuvant pain relief treatments alongside analgesics.
Additionally, there are limited studies on non-pharmacological pain management in children, making it challenging for therapists to justify children's participation and continued involvement in studies of this nature.
Also, the study's focus is on children with specific conditions (abdominal mass and acute lymphoblastic leukemia), which may restrict the applicability of the results to other cancer types or populations.
The lack of investigation into the effects of the three interventions (hypnotherapy, relaxation therapy, and music therapy) in combination with conventional analgesics which could limit the understanding of their potential synergistic effects.
LIST OF ABBREVIATIONS
| MT | = Music Therapy |
| VAS | = Visual Analog Scale |
| PMR | = Progressive Muscle Relaxation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study protocol was approved by the Ethics Committee of the Kurdistan University of Medical Sciences (code: IR.MUK.REC.1396.15), and the study has been registered on the IRCTID. Website: http://irct.ir (Code: IRCT20120905010744N2).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
The research objectives were explained to the subjects verbally and in a written manner, and written informed consent was obtained before enrollment. Notably, the participants were allowed to withdraw from the study at any given time.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Zenodo Repository at https://openpublichealthjournal.com/availability-of-data-materials.php.
FUNDING
The study was funded by Kurdistan University of Medical Sciences, Funder ID: IR.MUK.REC.1396.15.

