All published articles of this journal are available on ScienceDirect.

Physiotherapy Interventions and the Outcomes for Complex Regional Pain Syndrome (CRPS) Type 1 on the South Island of New Zealand – A Longitudinal, Prospective Case Series
Abstract
Physiotherapy is considered in pain medicine to be a key element in the management of Complex Regional Pain Syndrome (CRPS). This is the first paper to document and categorise all physiotherapy intervention methods used as well as evaluate the outcomes of a case series of 18 CRPS patients attending physiotherapy in a prospective, longitudinal study across a region. Outcomes were measured across the region of the South Island of New Zealand over 1 year through independent telephonic interviewing of the pain experience with the McGill Pain Questionnaire-short form, function with Foot Function Index for the lower limb or Disability of the Arm Shoulder and Hand for the upper limb, and quality of life with the World Health Organisation Disability Schedule. Clinical records were accessed for each CRPS participant following discharge from physiotherapy to categorise the intervention methods used. Seventeen participants received intervention for both functional restoration with pain modulation and only one participant received functional restoration with no pain modulation; 12 also received immobilisation with 10 receiving passive interventions. All outcome measures improved significantly by 6 months and were maintained at 1 year. Eighty five percent had their diagnosis of CRPS confirmed within 3 months of their injury; half had fracture as the precipitating injury for their onset of CRPS with a third following soft tissue injury and 11% following surgery. Physiotherapists showed a high variation with the intervention methods used and showed a greater proportion of intervention methods focusing on functional restoration followed by pain modulating interventions. Future research is necessary to define what physiotherapy interventions are efficacious in the management of CRPS.
INTRODUCTION
Complex Regional Pain Syndrome (CRPS) is an uncommon pain syndrome characterized by persistent regional pain that is disproportionate in time or degree to the usual course of any known trauma or other lesion [1]. CRPS may occur at the time of an injury, subsequent to an injury or occur spontaneously [2]. A distal predominance affecting the limbs with abnormal sensory, motor, sudomotor, vasomotor, and/or trophic findings is usual, with the syndrome showing variable progression over time [2-5]. The Budapest criteria are the most accepted criteria for the diagnosis of CRPS, where Type 1 is defined as no definitive nerve lesion and Type 2 as associated with a nerve lesion [6, 7].
It has been suggested that physiotherapy is an essential element in the management of CRPS [1, 4, 8-10]. Despite this, there is little research detailing the mechanisms how physiotherapy contributes to the recovery from CRPS [10], nor strong evidence for the safety or effectiveness of physiotherapy management of CRPS in clinical practice.
Unfortunately, reference in the published literature to “usual physiotherapy” of CRPS patients seldom contains details about intervention methods used [10-12].
The aims of this paper were to describe the natural history of 18 CRPS Type 1 patients living in the South Island of New Zealand (population ~ 1 million, area 150 437 km2) [13] for one year after starting physiotherapy; to document; categorise the physiotherapy interventional methods that they received and measure the patient outcomes.
METHODS
Participants and Recruitment
There are 150 private practices and hospital outpatient departments listed across the South Island of New Zealand as members of the New Zealand Physiotherapy Society (PNZ) or indexed in the telephone directory. Each practice was contacted to find out whether they accepted CRPS patients and would be willing to enrol any patients identified between February 2014 and February 2016 into the study. Treating physiotherapists were asked to;
- Assess patient eligibility and conduct informed written consent for the researcher to interview the patient and access to their clinical record (written consent was provided by a parent or guardian if patient was younger than 18 years),
- Provide the researcher access to their clinical notes to extract and categorise intervention methods used,
- List the autonomic changes observed and reported,
- Continue treatment as normal.
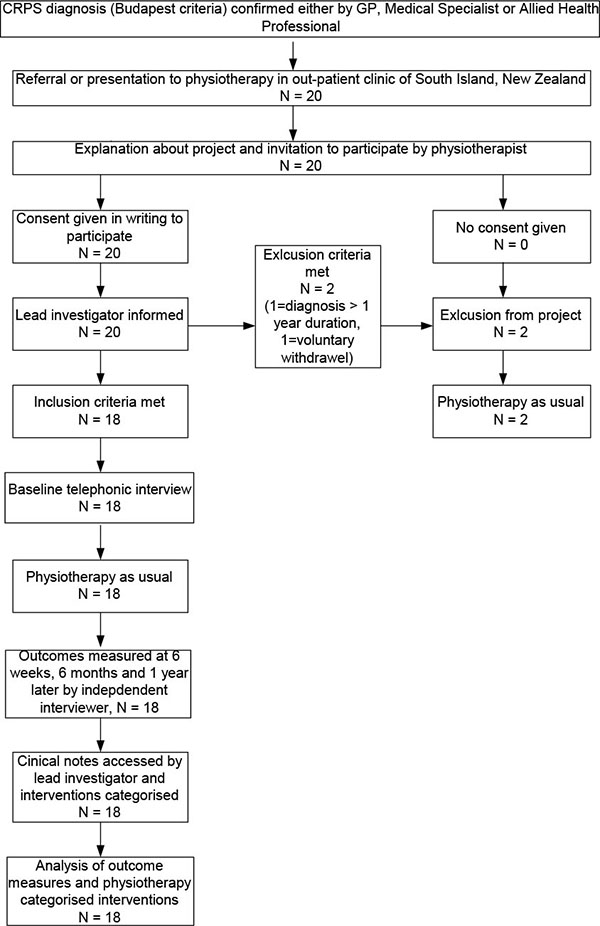
Participant inclusion criteria were a confirmed diagnosis by either General practitioner, Medical Specialist or Physiotherapist of CRPS according to the Budapest criteria [6] within one year of presenting to the treating physiotherapist. Potential participants were excluded if their CRPS diagnosis had been longer than 1 year; they had a terminal co-morbid condition; were blind (sight was necessary for graded motor imagery); or were unable to communicate in English or Maori (including deafness and cognitive impairment). Ethical approval for this study was provided by the University of Otago Ethics committee (Reference number H13/103, and ethical approval was granted from each individual South Island regional District Health Board.
Procedures
Upon receipt of signed consent, the researcher contacted each participant by telephone, explained the project, confirmed eligibility, and commenced the baseline measures. Baseline measures included age, gender and ethnicity as defined by Statistics New Zealand [14], as well as details about the initial event precipitating injury or pain, and time from first experience of pain to; (i) CRPS diagnosis; (ii) first physiotherapy intervention; and (iii) first pain medical specialist consultation.
The following outcome measures were also assessed at baseline and by independent interviewer at 6 weeks, 6 months and at 1 year. Pain intensity was measured using the Short form McGill Pain Questionnaire (SF-MPQ), an easy to administer scale [15, 16] widely used in CRPS research [17]. The SF-MPQ consists of 15 items that sum to form the Pain Rating Index (PRI), one item that measures Present Pain Intensity (PPI), and an 11-point Numerical Rating Scale (NRS). Functional ability was assessed using the 11-item Quick Disability of the Arm, Shoulder, Hand questionnaire (QuickDASH) [18-20] for those with CRPS of the upper limb, and the 23-item Foot Function Index (FFI) [21, 22] for those with CRPS of the lower limb. Quality of life associated with disability was assessed using the 12-item World Health Organisation Disability Assessment Schedule 2.0 (WHODAS 2) [23], which was chosen as appropriate for both upper and lower extremities.
Following the last interview, the treating physiotherapist(s) were contacted and clinical notes were accessed by the researcher to determine the type, frequency, and duration of interventions administered as well as clinic non-attendance. Physiotherapy treatment interventions were categorised into one of five by an experienced Physiotherapist and a Pain Specialist Physician according to the “target” of the intervention; where functional restorative target active joint range of motion, muscle strength, balance and proprioceptive exercise; pain modulation target central processing; immobilisation restricts or inhibits any active activity and passive interventions require no active engagement of the participant with the intervention:
- Functional restorative interventions (TIF): active, passive, resisted, balance or proprioceptive land based exercise with time contingent homework prescribed.
- Pain modulation interventions (TIP): Graded Motor Imagery (GMI), mirror exercise, pool exercise, Transcutaneous Electrical Nerve Stimulation (TENS), Cognitive Behavioural Therapy (CBT), acceptance and commitment therapy (ACT), problem solving, relaxation and breathing, Sensori-motor Training (SMT) including sensory mapping, and discrimination and desensitising with pain contingent homework prescribed.
- Education: a written record of “education”.
- Immobilising interventions (TII): bracing, splinting or taping.
- Passive interventions(TIP): massage (scar tissue, lymphoedema or oedema), acupuncture, ultrasound, and application of heat or wax bath.
Other interventions, both medical prescriptions or procedures and other allied or alternative health interventions were recorded from the participant’s interviews and verified with the clinical physiotherapy notes.
Statistical Analysis
Participant baseline characteristics and outcome measures were summarised using standard descriptive statistics. Paired student-t tests were used to test statistical significance (using a significance level of p < 0.05) of changes in outcome measures from baseline to one year. Analysis was performed using Statistica 7 and Microsoft Excel for windows PC.
RESULTS
Sixty-four (43%) of the 150 physiotherapy practices or outpatient clinics contacted reported that they accepted CRPS patients, and fifty seven of these (89%) indicated they were willing to recruit patients into the study. Twenty CRPS patients signed consent to participate, but one was excluded due to their duration of CRPS greater than one year at consent and one withdrew for personal reasons. All follow up measures were completed for all participants. Fig. (1) represents the flow chart of recruitment for participants and clinical records for this project.
Participants were predominantly New Zealand European (Pakeha) female with a wide age range (11 to 72 years); from mid and north Canterbury where the greatest population density lives; the education equivalent of completed school years; half with a fracture injury which precipitated their CRPS; the upper limb affected more often (68%) than the lower limb and most (85%) had been diagnosed within the past three months. Participant baseline demographic and clinical details are reported in Table 1.
| Characteristics | N (%) |
|---|---|
| Age in years, Mean (SD) [range] | 43.9 (19.5) [11 to 72] |
| Gender Female Male | 16 (88%) 2 (12%) |
| Ethnicity New Zealand European (Pakeha) Maori Pacific Other | 15 (82) 1 (6) 1 (6) 1 (6) |
| Education number of years, Mean (SD) | 13.5 (3.3) |
| Region, from south to north Southland Otago Mid and North Canterbury South Canterbury Nelson/Marlborough | 2 (11) 2 (11) 12 (68) 1 (5) 1 (5) |
| CRPS precipitating event Fractures Soft tissue injury Surgery | 9 (53) 7 (37) 2 (11) |
| Affected limb Upper limb Lower limb | 13 (68) 5 (32) |
| Laterality Right center | 10 (53) 8 (47) |
| Time to diagnosis from injury 1-3 months 3-7 months | 16 (85) 2 (15) |
Physiotherapy Interventions
The eighteen participants summed a total of 365 physiotherapy sessions (median = 16.5 sessions, IQR = 8-33), involving 274 contact hours (median = 13, IQR = 4.3 - 19.4). Participants on average attended physiotherapy for median 20 weeks with Physiotherapy interventions had been completed by 6 months for 10 participants’ (55%) and three (17%) had self-discharged by this time. One more participant was discharged by their one year interview leaving 4 (22%) engaged with ongoing Physiotherapy. The number of physiotherapy sessions attended and number of contact hours with the Physiotherapist had large interquartile ranges from their respective medians, namely 20 (14) and 15 (13), respectively. These are shown in Table 2.
| Self-discharge | Discharge by Physio | On-going Physio | Whole Sample | |
|---|---|---|---|---|
| N = 3 | N = 13 | N = 2 | N=18 | |
| Total no of physio sessions attended, median (IQR) | 7.0 (3-17) | 16.0 (8-30) | 42.0 (39-45) | 16.5 (8-33) |
| Total no of contact hours with physiotherapist hours, median (IQR) | 4.3 (2-17) | 12 (4.5-17)) | 36.2 (33.4-39) | 13 (4.3-19.4) |
| Total duration of weeks of physiotherapy, median (IQR) | 12 (4-16) | 20 (16-32) | 38 (32-44) | 20 (16-32) |
Physiotherapy categorised interventions for participants were collated. Seventeen participants received intervention for both functional restoration with pain modulation contributing to 55% of all interventions applied and only one participant received functional restoration with no pain modulation intervention; 12 received immobilisation and 10 received passive interventions. Data at 6 weeks showed a slightly greater use of pain modulation than functional restoration intervention but by one year it showed the total percentage of modalities focused around improving function (42%) was greater than the percentage of interventions focusing on modalities for pain modulation (34%). All received a record of education but this was documented at most only once a week. The average weekly numbers of interventions for each category tended to decrease over time. Data is shown in Table 3.
| Category of Intervention |
Intervention total N, mean (SD) Interventions per week, mean (SD) |
Percent of all Interventions | |||
|---|---|---|---|---|---|
| 6 weeks | 6 months | 1 year | Total | ||
|
Functional Restoration N= 18 |
22 (13) 3.7 (2.1) |
44 (43) 2.4 (2.4) |
8 (15) 0.4 (0.6) |
74 (60) 1.4 (1.2) |
42 |
|
Pain Modulation N= 17 |
24 (28) 4 (5) |
27 (38) 1.5 (2.1) |
7 (15) 0.3 (0.6) |
59 (73) 1.1 (1.4) |
33 |
|
Functional Restoration and Pain Modulation N=17 |
46 (32) | 71 (70) | 15 (29) | 97 (68) | 55 |
|
Education N= 18 |
6 (4) 1.1 (0.7) |
8(8) 0.5 (0.5) |
2 (3) 0.08 (0.1) |
16 (13) 0.3 (0.2) |
9 |
|
Immobilisation N=12 |
5 (8) 0.8 (1.3) |
9 (18) 0.5 (1.1) |
1 (5) 0.05 (1.2) |
15 (29) 0.3 (0.6) |
9 |
|
Passive N=10 |
4 (8) 0.7 (1.3) |
8 (14) 0.4 (0.7) |
0.7 (1.8) 0.03 (0.08) |
13 (18) 0.3 (0.4) |
7 |
Outcome Measures
Mean scores for the outcome measures of the SF-MPQ, WHODAS, FFI, and QuickDASH all showed significant improvement with a clinically important change with the reduction by half the baseline score at 6 months. A statistically significant improvement is shown to be maintained at 1 year but FFI was the only scale to show continued improvement after six months Table 4.
|
Outcome dependent variable (Score range, clinically important change) |
Baseline score, mean (sd) N = 18 |
Change at 6 weeks, mean (sd) N = 18 |
Change at 6 months, mean (sd) N = 18 |
Change at 1 year, mean (sd) N = 18 |
t-test P (change at 1yr) |
|---|---|---|---|---|---|
|
SF-MPQ PRI (0 to 45, >5) |
21.8 (8.1) | -9.4 (9.9) | -15.6 (10.7) | -15.6 (12.2) | <0.001 |
|
SF-MPQ NRS (0 to 10, > 3) |
6.4 (1.6) | -3.0 (2.6) | -4.4 (2.8) | -4.6 (2.8) | <0.001 |
|
WHODAS (0 to 60, > 15) |
80 (22.5) | -27.3 (28.1) | -47.3 (26.7) | -47.1 (34.8) | <0.001 |
| N = 5 | N = 5 | N = 5 | N = 5 | ||
|
FFI (0 to 100, >10) |
47.6 (12.1) | -20.47 (13.0) | -29.5 (14.2) | -39.9 (21.1) | 0.02 |
| N= 13 | N= 13 | N= 13 | N= 13 | ||
|
QuickDASH (0 to 100, >15) |
60.0 (18.5) | -31.3 (25.6) | -43.4 (21.2) | -39.7 (21.0) | <0.001 |
DISCUSSION
These data provide the first contribution to the literature about physiotherapy interventions used for management of CRPS in clinical practices across a region. The characteristics of this case series sample show a predominantly female Pakeha (New Zealand European) group with an age range from 11 to 72 years. CRPS is shown to affect all age groups with the greatest risk being the post-menopausal female [24]. The average education level was 13 years, involving completion of an equivalent schooling qualification. Almost seventy percent were from the region of the greatest population density, mid/north Canterbury. Half had fracture as the precipitating injury for their onset of CRPS with a further third following soft tissue injury and a small group of 11% following surgery. Laterality of affected limb was almost equally shared between left and right sides and most (68%) had their upper limb affected.
This case series shows 85% to have had their diagnosis of CRPS confirmed within 3 months of their injury and that all outcome measures improved significantly by 6 months and were maintained at 1 year. This supports the evidence that early diagnosis can improve outcomes [9, 25]. Clinically important changes are represented in the QuickDASH as a change of 15 points [26]; WHODAS as 15 [27]; MPQ PRI as 5 with NRS as 3 [28]; FFI as 10 [21]. This sample shows significant clinical improvement across all measures 6 months after commencing physiotherapy. The FFI shows continued improvement between 6 months and 1 year while the QuickDASH deteriorated slightly despite still maintaining significant improvement from baseline measure. Fifty-five per cent had completed their physiotherapy intervention by 6 months later with a good outcome. Only 2 required ongoing physiotherapy care and their outcomes were also improved by this time. However, three patients self-discharged from physiotherapy and chose alternative therapies (2 chose Neuro-linguistic programming and 1 would not disclose his intervention) and their outcomes improved despite their non-attendance. It is shown that CRPS can resolve spontaneously for a small sub group [29].
This sample shows that the outcome measure improvement is despite a widely varied duration or category of physiotherapy intervention(s) used. It supports the optimistic outcomes with tailored intervention [30-32], yet it is also possible that the improvement seen with this case series is simply regression to the mean. Other publications [33-36] document physiotherapy and that the CRPS problems improve, but this is the first to record and categorise every physiotherapy intervention used across a region and evaluate the respective outcomes. The outcomes measures all show a significant improvement with reduction by at least half the baseline score which is shown to be a clinically meaningful change. The sample size is, however, too small to make any definite conclusions regarding the efficacy of any specific intervention used. It is noted that for this sample a slightly greater percentage of interventions focussed on both functional restoration as well as pain modulation. The effect is not possible to determine with this small sample size. It is also possible the different physiotherapy interventions could be categorised differently. Furthermore, it is not possible to determine those CRPS patients who did not present for physiotherapy, or presented to other health care providers, or who simply self-managed their problem without interacting with any health service. The first epidemiological publication on CRPS noted that 93% of the CRPS population did attend physiotherapy and 87% reported about physiotherapy being efficacious [29]. The effect of attending physiotherapy, or not, is yet to be explained [29, 37-41].
These data illuminate a possible conflict that influences the physiotherapist’s management of CRPS patients. A dichotomy exists in the literature showing that persistent pain can be aggravated by activation due to temporal summation [42]; yet the population who exercise more regularly experience less persistent pain [43, 44]. Many CRPS patients present with reasonable functioning, but continue to experience severe pain despite persevering with exercise [45]. Management for CRPS remains difficult; the clinical presentation of CRPS remains highly variable [46]. Hence, to simply normalise function does not necessary reciprocally reduce the pain experience or vice-versa. Ethically, it is not possible to deny treatment, and which intervention method and at what dose is urgently needed to be determined for the different presentations of CRPS. Importantly also, to explore why some self-discharge or do not attend physiotherapy and what constitutes their subsequent improvement is crucial. There is at present no algorithm for what physiotherapy intervention(s) are essential for the physiotherapy management of CRPS. Despite these difficulties, physiotherapy is recognised as an essential part in reducing pain and improving function in the management of CRPS [4, 8, 11, 47-50]. Other data report favourable outcomes for a sub group of CRPS patients [25, 38, 51, 52] which is consistent with this case series. However, it is reported that others recover poorly resulting in poor health and function [38, 45, 53-55].
A weakness of the study was its small sample size allowing potential bias to occur from both CRPS participants and five per cent of Physiotherapists who do manage CRPS patients did not engage with this study reflecting a possible skew reflection of usual physiotherapy applied for CRPS. The clinical notes of intervention accuracy are problematic, e.g. education is an integral part of the Physiotherapist’s conversation with any patient, yet the intervention of “education” was only recorded at most once a week. To obtain independent recorders of physiotherapy interventions was not possible for this study since it covered an area 150437 km2. Another potential recognised weakness of the study is the use of Likert scales for accurate statistical analysis of continuous variables.
This study’s strength is its originality to document and report data across a region for physiotherapy interventions with respective outcomes, minimal interviewer bias and valid self-reporting questionnaires [56]. There is a lack of good evidence as well as disagreement about which physiotherapy interventions are effective in managing the diverse presentations of CRPS. Future research is needed to determine a robust evidence based model for the physiotherapy management of CRPS and this paper is the first to provide a platform for comparison across a region.
CONCLUSION
This is the first record of physiotherapy for CRPS management and patient outcomes across a region. CRPS is not a common problem presenting to health professionals and this case series showed all outcome measures to show significant improvement after 1 year with intervention methods focusing primarily on functional restoration and pain modulation. There is a lack of strong evidence to determine which interventions are effective in a clinical setting for the diverse presentations of CRPS. Future research should define what physiotherapy interventions are efficacious in the management of CRPS.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No Animals/Humans were used for studies that are base of this research.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Thanks are extended to the New Zealand Pain Society for their grant given towards a contribution to the costs of an independent interviewer.
Thanks are extended to the Physiotherapists who referred their CRPS patients and allowed access to their clinical notes for the evaluation of physiotherapy interventions; Lucy Ireland, Rebecca Darby, Leigh Law, Neil Familton, Suzanne Black, Jarrod Watt, Clare Kiamtia, Sean Wilson, Miranda Buhler, Josh Woodside, Audra Cuellar and Trish Brown.

